|
A 34 year old male presented with central crushing pain for 6 hours. Onset was sudden, while cleaning the kitchen. The pain radiated to both arms. He had complained of some chest pain on exertion over the last 3 days, e.g. when climbing stairs. The chest pain did feel better when he sat forward, and worse when lying flat. PMH – he had been treated with omeprazole by the GP for the last 6 weeks for indigestion type symptoms. He was a smoker. On examination – pale, sweaty, in pain, apyrexial, BP 156/90, pulse 80. Heart sounds were normal. He had equal radial pulses. 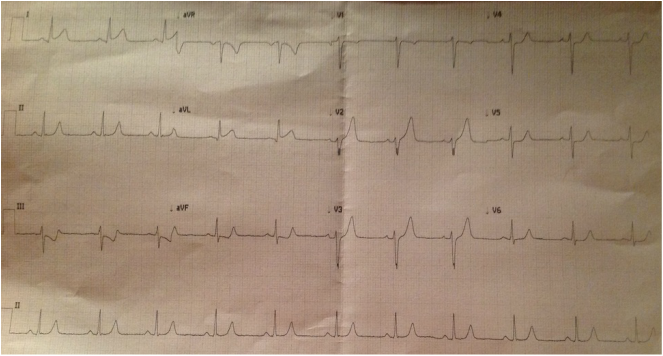
What's the diagnosis? The ECG shows ST elevation in I and aVL, but also significant ST depression in III, also some in aVF, V4 and V5.
He was taken straight away for diagnostic coronary angiography where they found severe disease to the LAD and a large branch of the intermediate artery was blocked at the origin, both of which required stenting. For those who were considering pericarditis, remember: Factors strongly favouring acute MI v pericarditis on ECG: ST segment depression (beyond V1 and aVR) ST segment convex upwards or horizontal ST Elevation III > II Remember AMI can also give a pericardial rub and the pain can be positional If you want the expert summary of Pericarditis vs STEMI, watch this.
0 Comments
Leave a Reply. |
|
|