|
I came across this really informative 10 minute session by my EM Cardiology and ECG hero, Amal Mattu. Well worth a watch:
Almost every medical student and trainee in almost every specialty is taught that one should always assume and treat any regular WCT as VT. The wisdom behind this conservative teaching is simple: If a patient with SVT-AC were misdiagnosed as having VT, the resulting therapies are generally safe and effective despite the misdiagnosis; but if a patient with VT were misdiagnosed as having SVT-AC, the therapies can be deadly, and the patient is shortchanged of an appropriate work-up. The ALS tachycardia algorithm give us a clear approach to these situations 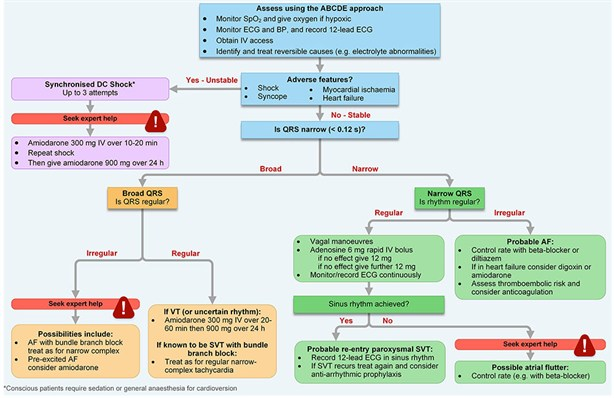 According to this algorithm, if we have a patient with a regular wide complex tachycardia (RWCT) and no adverse features, we could treat them with Amiodarone. Amiodarone has class I II III and IV anti-anti-arrhtyhmic actions - this means Na-channel blockade, beta blockade, potassium channel blockade and calcium channel blockade.
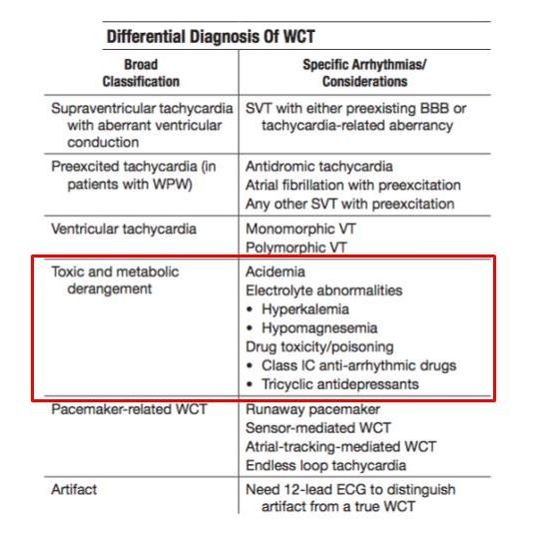
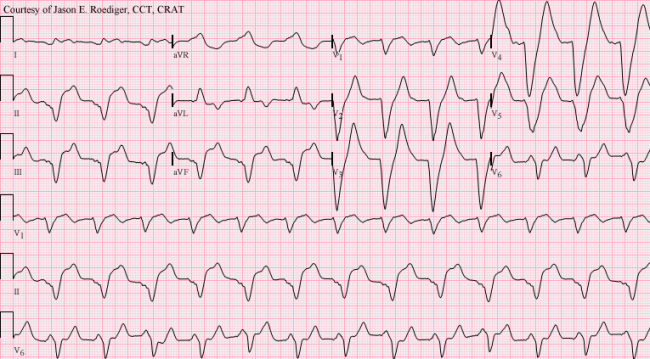 Take home message:whenever you see Regular REALLY Wide Complex Tachycardia (> 200 ms) consider toxic or metabolic derangement first and treat with Calcium Chloride / Sodium bicarbonate NOT Amiodarone (which is a sodium channel blocker and will lead to asystole in these cases). N Bothma
8 Comments
|
|
|