|
This is the presentation I gave at the ED Wellbeing day back in the summer. It is also available as a webinar on the Trauma Care website, and we discuss similar themes in this podcast. I have been inspired by several other people to produce this blog, and if you would like to know more I suggest you find them on Twitter, where you will find links to their FOAM resources: @emcrit, @DocTomEvens, @HumanFact0rz, @ResusPadawan, @EMSwami  Firstly I would like to emphasise that this blog is concerned with the ability to perform when faced with acute stress, not chronic stress or post-traumatic stress disorder.
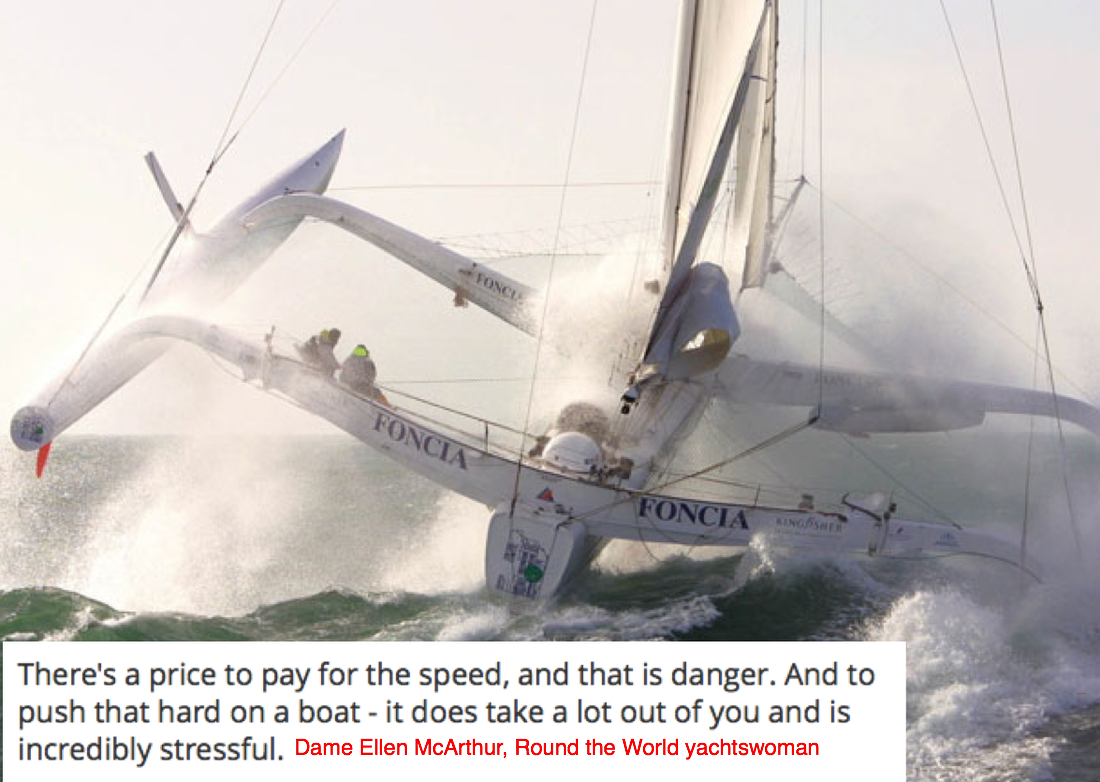
 The reason we, as humans, have a response to stress is the innate 'fight or flight' reflex which kept our ancestors alive. But the very design that gave us a survival advantage as cavemen, unfortunately has deleterious effects on our ability to perform under stress, when what we really want to do is run away!
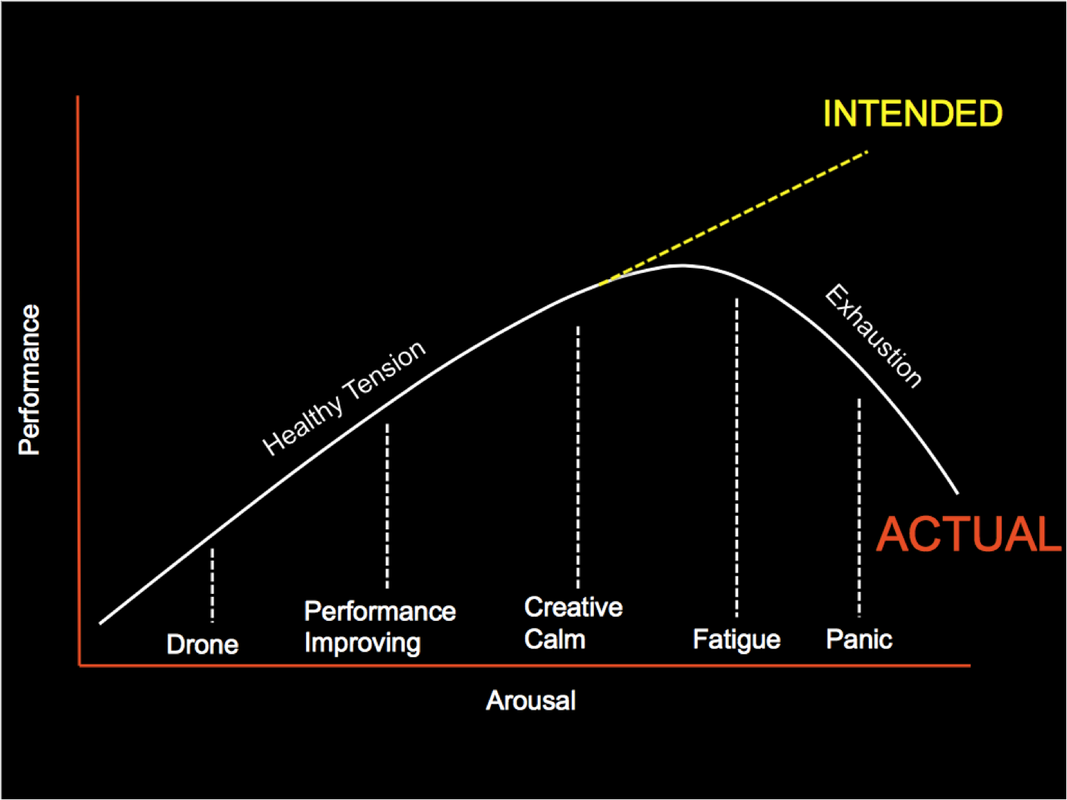
A little bit of stress is a good thing?In 1908, Robert Yerkes and John Dodson presented their ground-breaking research on the non-linear nature between arousal, based on task difficulty, and brain functioning. Focused/in-the-zone is a good thing. Performance improves when you are ‘a little bit activated’. But we need to be aware that this is not exponential – and recognise when performance tapers off.
There is a really interesting book on this subject by Lt. Col Dave Grossman, called 'On Combat'. It discusses the effect of stress on performance in the context of ‘deadly force encounters’ amongst military and armed police, and provides huge insight into the way in which stress could affect performance in medical staff too. Listen to this Emcrit podcast to hear more. 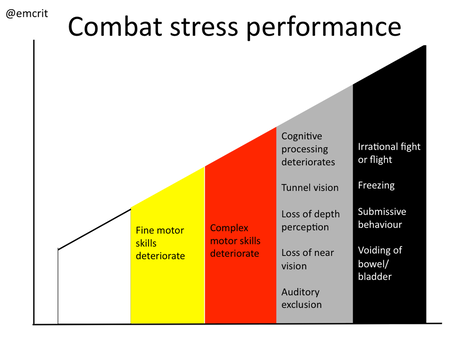 Performance Deterioration as a Function of Heart Rate From On Combat, by Lt. Col Dave Grossman – former US Army Ranger & paratrooper
 The deleterious effects of stress on performance are profound and pervasive. The time taken to complete manual tasks is doubled under stress conditions. In addition to the physiological consequences of increased heart rate, breathing rate and tremor, there is also an emotional and cognitive burden.  We feel fear, anxiety, frustration, and lose motivation. We have a narrowed attention, decreased search behaviours, longer reaction time to peripheral cues, decreased vigilence, degraded problem solving, performance rigidity. There are changes in social behaviour: loss of team perspective, decrease in pro-social behaviours such as helping, obliterate ability to share mental model. Acute stress causes a doubly-whammy in terms of potential error, it erodes decision-making and situational awareness, and reduces team performance; so the individual is less receptive to suggestions from others, which would normally provide a safety-net. Why do we feel stressed?Before we can enhance our performance, we need to understand what causes us stress. 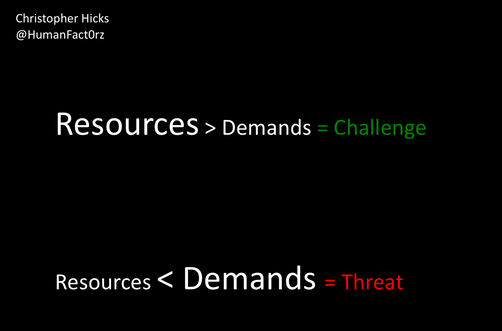 A process occurs by which environmental demands (eg performing in front of others, taking an exam) evoke an appraisal process in which perceived demand exceeds resources, and results in undesirable physiological, psychological, behavioural or social outcomes. If the individual determines that his or her resources are sufficient to meet the demands of the situation, the situation is appraised as a challenge and the potential for gain (i.e. elevated self-esteem, learning) is recognised. If the resources are not judged to be sufficient, the situation is appraised as a threat because of the significant potential for loss. Socio-evaluative stressors (when behaviour is potentially judged by others) and uncontrollable situations are more likely to be appraised as threats than challenges. What can we do about it? In advance...We need to move into a Challenge rather than a Threat mindset. Think about how you can increase your resources:
 Stress inoculation training (SIT) is a three-phase cognitive behavioural training approach to limit the impact of acute stress on performance. SIT has been used to decrease the perception and influence of stress – or promote ‘stress resistance’ – across a variety of domains, from public speaking to combat aviation. Have a read of this blog/listen to the podcast for more information. 1. Conceptualisation-give a background of stress responses, why they happen, and what to expect. 2. Train and educate on the skills and tasks we want to see performed under stress. Then give the tools to deal with the expected stress. 3. Do a dry run to train in simulation without added stressors 4. Run the same training with stress inoculation  Your brain is the most powerful simulator you have. Mental Practice is the mental rehearsal of activity in the absence of gross muscular movements; it has been demonstrated to enhance acquisition of technical and procedural skills. It has been shown to improve performance in basketball and piano players, to a standard equivalent to them having physically practiced performing the procedure, and there is evidence to support the same in the medicine. What can we do about it? On the day... Tactical breathing. Take a deep breath in for 4 seconds, hold it for 4 seconds, breath out for 4 seconds, hold for 4 seconds. Repeat. This combats the physiological affects of stress, and moves you down the combat stress performance graph.  Positive self-talk is used by athletes and any elite performance group. Visualise yourself performing the task exactly how you want to see it done. Your own perceptions are important: Recognise your own stressors, beware of going into it with negative thoughts Think about when you did it well, visualise success Change your negative into positive thought (exude confidence, for both your patients and your trainees) 'Calm is contagious' Accept the fact, but reject the premise. Yes I was unsuccessful last time I performed this procedure but that doesn't mean I cannot be successful this time. 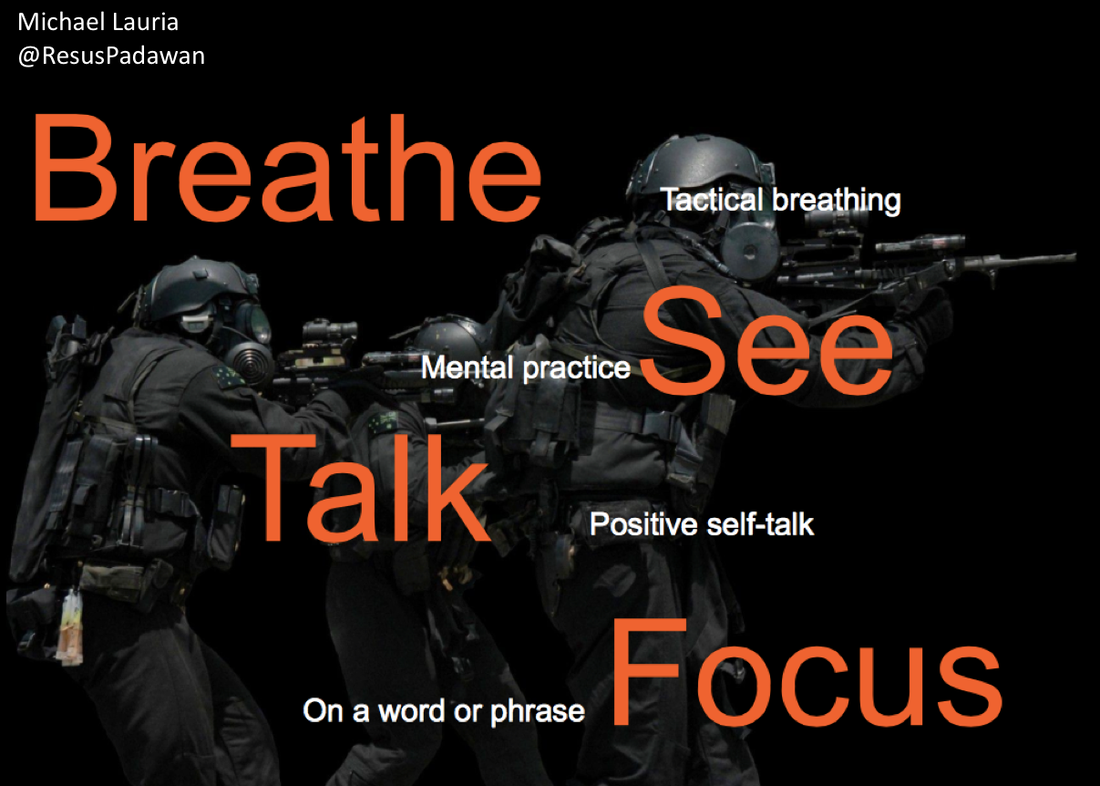 C Bosanko
6 Comments
What is anxiety? It is a psychological and physiological state characterised by somatic, cognitive and behavioural components. And it is a BIG problem....
 I suppose this is not surprising, and our Emergency Department is just as bad, if not worse, than an anaesthetic room: it is an alien environment, there is lots of frightening equipment stuff, and people rushing about! Children may be pushed beyond their capacity to cope. 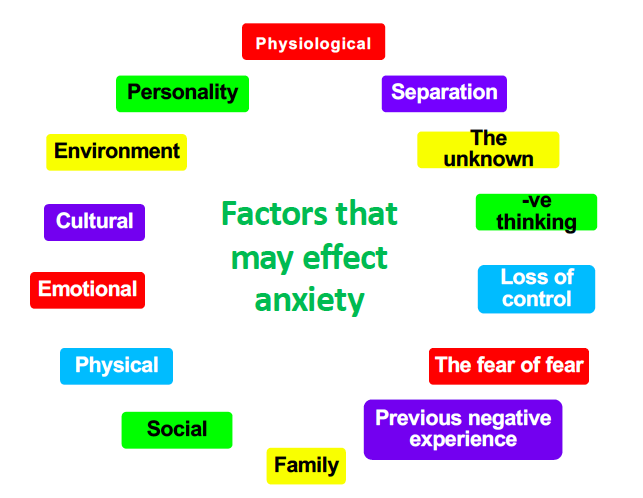 Our job is to help children cope with anxiety and reframe it so that it does not become crippling. But how? Communication is key.
Advanced communicationAdvanced communication techniques fall into two groups
Control attention Overload Example: "Hello James, come in. I love your shoes, reckon they'll fit me? I reckon they're too small but what's size between two friends? I'd probably bend them if I wore them, but not like Beckham though. He's a good player, better at United than Real, the real deal in red not white I think. Red devils are United, but they're heavenly players, making music on the pitch, perfect pitch but I'm tone deaf even though I love to sing in the shower. Not the rain shower, though Singing In the Rain is a great film, but water in the camera is bad news, it makes the colours run off the screen, right off track but listen to me I'm like a stuck record." Accelerated rapport Behaviour, non-verbal, verbal or tactile usually associated with having rapport where as yet that rapport does not exist. Yes set
Bind of comparable alternatives Free choice of two or more comparable alternatives, and whichever is chosen leads to behaviour in the chosen direction. Usually feel bound to accept one alternative.
Coping strategies Humour Use with caution and be inclusive and appropriate
Successive approximation
Distraction therapy Methods to reduce anxiety and pain by focusing on something else
C Bosanko
|






|
|