|
Today we tried something different in a sim session… O&G Consultant Tim came down to ED with two of his registrars (Steph and Amy) and we rotated through two obstetric emergencies in ED stations… socially distanced of course but let me tell you, there is NOTHING socially distanced about the raw practice of delivering a baby! Amy and Steph talked us through a normal delivery:  Should present face down, deliver the head, then allow “Restitution” – where the baby rotates to fit the torso through the birth canal. On the next contraction – the anterior(upper) shoulder should deliver then posterior shoulder. Now breathe yourself…. And if the baby is breathing – there is no rush to cut cord, you can give the baby a quick dry and a rub and put it skin to skin with mum… job done! Then, we talked through and delivered a baby with the absolutely EMERGENCY finding of Shoulder dystocia… code very, very scary… This is where the baby’s shoulder is stuck behind mum’s symphysis pubis… Risk factors – obesity in mum, gestational DM – big baby Head may deliver slowly, ‘turtle necking’, undelivered chin. May not restitute fully No progression on second contraction This is completely Time critical– as a team we have only a few minutes to prevent a hypoxic brain injury/death… here is the SOP:


Be aware that you may cause fractures to humerus/clavicle, this is totally OK if you can baby out alive…. Super scary… let’s hope those 2222 bleep holders can run fast and have mini, super strong hands!! Give this a watch: https://www.youtube.com/watch?v=1HeXmlf_sp4 Our obstetric registrar friends also talked us through how to deliver a baby presenting as a Breech delivery… First thing: This May be very quick in multiparous women – be prepared to catch!  You will notice that buttocks are presenting. The baby is facing posteriorly (down)… Bring mum to the end of bed. This is a hands off situation. Minimal handling of the baby will avoid stimulation that will promote breathing (while head still inside)/increased metabolism/oxygen consumption. If handling is required - only to the bony pelvis/hips of the baby. Allow the buttocks to deliver – allow baby to hang down The hips will probably be flexed and knees extended, you can use your finger to ‘flick’ them out: 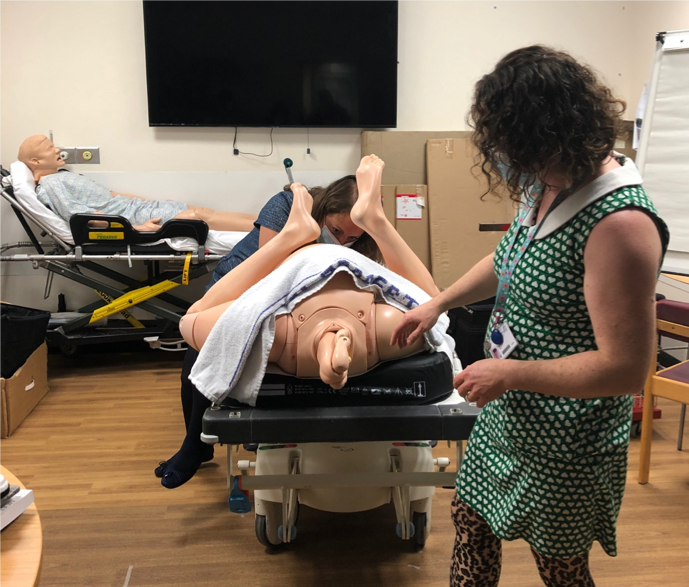 Allow delivery until the shoulder blades are seen The arms can be delivered by gentle rotation of baby at hips Or Sweeping the arms over the baby’s face with a finger 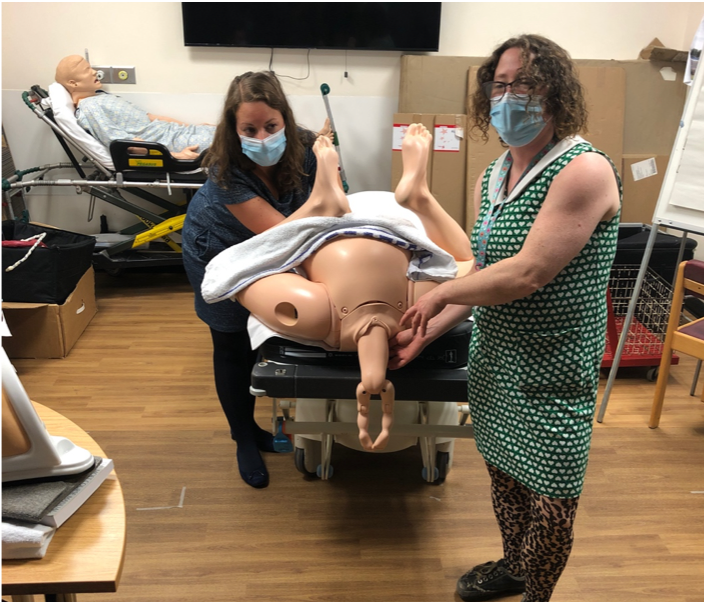 The neck/head needs to flex to allow narrowest cross section to pass through the birth canal.
 Again, have a watch of this: https://www.youtube.com/watch?v=EWjKswZ3Mm8 And that if that didn’t get our hearts racing fast enough, we also spent an hour chatting to Tim about resuscitating the pregnant patient in a peri-arrest or cardiac arrest situation, medications during pregnancy, post partum haemorrhage management and pre-eclampsia treatments… The harsh fact is maternal mortality is not falling, despite improvements in care because patients are becoming increasingly complex…  While we work at Derriford ED, we need to know a few things about obstetric emergencies: 30993 – Labour ward emergency phone – useful if putting out a 2222 – tell them what the problem is – so they know what to bring eg – shoulder dystocia (run very, very fast and get here yesterday) vs PPH (come quickly). As a refresher, we reminded ourselves of the physiological changes that occur in pregnancy, affecting every letter from A-E… check out the PROMPT course for more on that or read your ALS special circumstances chapter… Here area few pearls from Tim’s talk:
Resuscitation in pregnancy…also a scary subject… Same principles as any other resuscitation but do not forget:
Now the thorny subject of PE/VTE disease in pregnancy…. A negative D-dimer is probably useful in low pre-test probability patients but what about imaging?? V/Q vs CTPA
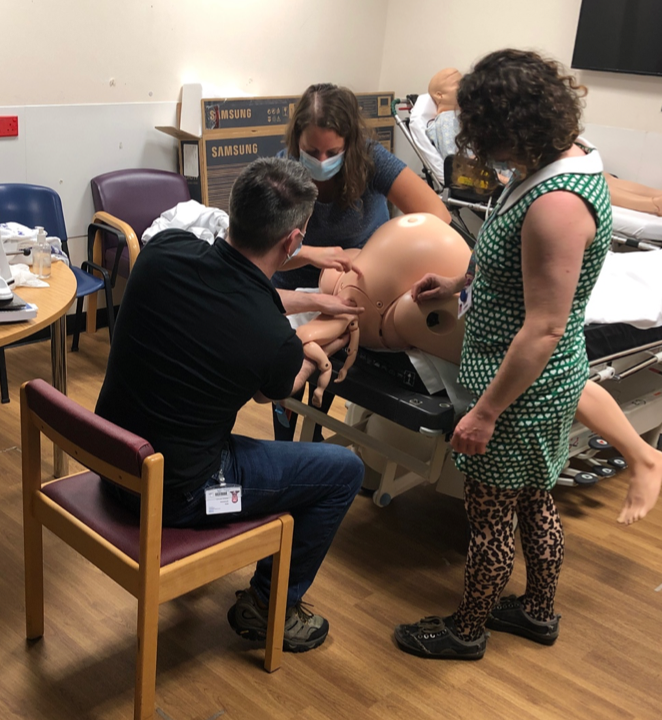
We had a great chat about managing Post-Partum Haemorrhage (PPH) Primary PPH occurs up to 48 hours of delivery vs Secondary PPH which occurs after 48hours (secondary is much more likely to be infective) Resuscitate – as for haemorrhagic shock – think blood products, rotem, calcium etc. Give antibiotics if suspected infection (so nearly all secondary PPH)… We all love the 4Hs and 4Ts of cardiac arrest causes… but in obstetrics, let’s not forget the 4 T’s of PPH: Tone– Most common, the uterus is exhausted after its big night out (push,push, push) and needs a hormone to increase uterine contraction – ergometrine/syntometrine/misoprostil. (caution if hypertensive). We keep ergometrine in our ED resus drug cupboard:  Tim also reminded us about using Bimanual compression in these ladies: put a fist into the vagina while also applying fundal pressure – it should be painful/tiring if effective (may need to change operator). Here is Tim showing us the desired effect on the tired atonic uterus….  On those 4Ts also think:
Trauma–a simple perineal tear possibly… – if arterial, can bleed quickly – fresh red blood is likely to be perineal: is it possible to put a quick suture in place and apply pressure? Tissue– Retained products? Check the placenta after eth delivery of the baby and placenta, is there a chunk missing or ragged membranes, suggesting some may remain in mum’s uterus? And finally: Thrombin– Are they forming clots? – A DIC picture represents fairly advanced bleeding… we need ROTEM to help us… along with the expertise of the obstetric team… resuscitate with blood products asap. Briefly, we considered another obstetric emergency presentation we may see in ED: Eclampsia Usually we will see a patient presenting with a headache and Hypertension and/ or proteinuria (can occur without either but very rare). This is pre-eclampsia… It is of unknown cause but may progress to seizures – give MgSO4 - 4g in 20mls saline over 20 mins (double the typical ED dose for asthma etc) Use labetalol for BP control…. And that was our multiprofessional interactive, hands on, socially distanced morning…. More soon, watch this space! With huge thanks to the obstetric team of Tim, Amy and Steph, to James Keitley for his unwavering enthusiasm for education and awesome administrative support today and to Neil Spencer for lending me his notes to Annetticise…
2 Comments
James
7/11/2020 12:43:25
Awesome summary, thanks Annette!
Peter Filser
15/11/2020 15:09:42
Thank you so much for this summary. Very helpful. Leave a Reply. |
|
|