 ACCS teaching this week was on the topic of Vertigo & dizziness, we thought it would be useful to share some key points with a wider audience, and point you in the direction of some great resources, particularly the RCEM Learning module on the topic What do patients mean when they say 'I feel dizzy'?1 Vertigo an illusion of motion of either the subject or the environment 2 Presyncope a feeling of impending faint or loss of consciousness 3 Disequilibrium impaired balance and gait in the absence of abnormal head sensation dizziness of the feet 4 Light-headedness a non-specific description of symptoms that cannot be identified as one of the above types 3% of patients present to ED with dizziness/lightheadedness/imbalance, which equates to approximately 9 patients per day to our department, and the literature states that up to 28-59% of posterior strokes are missed in the ED. VertigoVertigo is defined as an illusion of rotatory movement and always implies an imbalance in the vestibular system although the symptom doesn’t indicate where the imbalance originates. Around half of patient presenting with vertigo have peripheral cause. Anatomy & pathophysiology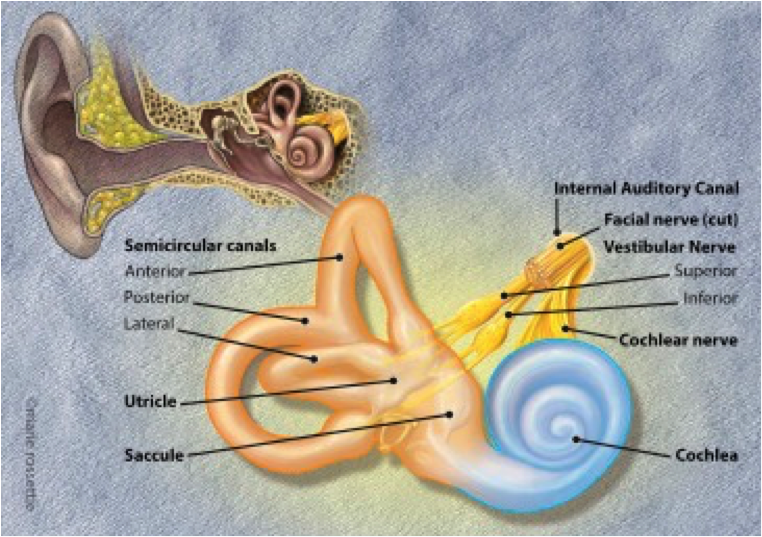 Sensory inputs from the vestibular apparatus, visual system and proprioceptive stimuli from the neck and rest of the body. The vestibular apparatus consists of the membranous labyrinth contained within the bony labyrinth lying in the petrous temporal bone, which connects via the vestibulococclear nerve to the vestibular nuclei in the brainstem. These nuclei interconnect with neurones in the cerebellum, spinal cord and cerebral cortex. The membranous labyrinth consists of the three semicircular canals and two chambers, the saccule and utricle. Flow of fluid (endolymph) in the canals stimulates cilia attached to a sensory organ located in the ampulla of each canal, the crista ampullaris. In the saccule and utricle, movement of calcified calcium carbonate crystals (statoconia or otoliths) stimulates cilia of another sensory organ, the macula. Therefore movement of the head in any plane modifies neural impulses transmitted via the vestibular nerve, connected to each of the sensory organs, to nuclei in the brain stem. Vertigo results from an imbalance of either the received signals or information processing in the brainstem. Vascular supply is from anterior inferior cerebellar artery and posterior inferior cerebellar stray. These are branches of the basil artery and vertebral artery - the posterior circulation. When assessing a patient with dizziness...Establish that it is vertigo and not one of the other symptoms. A multitude of medical problems can cause lightheadedness/presyncope - these need to be explored and investigated differently (VBG/ECG/BP will be useful in this regard). History 1. Onset: rapid vs insidious 2. Associated symptoms e.g. nausea/vomiting (more common in peripheral causes), tinnitus + deafness (both suggest Menieres) 3. Effect of head position on symptoms: exacerbated movements of head and then settles (suggests BPPV), exacerbated by movements of the head but persist (labyrinthitis, vestibular neuritis), not affected by movement of the head (central cause) 5. Recent local trauma (consider possibility of vertebral artery dissection if any preceding neck pain) or infection 6. PMHx: particularly for stroke risk factors 7. DHx: ACE inhibitors, amiodarone, aminoglycosides, beta blockers, cocaine, phenytoin, salicylates, sildenafil may all cause vertigo Examination 1. Ataxia (suggest central cause) 2. Nystagmus: Peripheral – horizontal, fatiguable, surpressed on visual fixation, unidirectional, fast phase beats away from pathology 3. Cranial nerves, including hearing assessment 4. Peripheral nervous system 5. Check for cerebellar signs (DANISH = Disdiadochokinesis, Ataxia, Nystagmus, Intention tremor, Slurred speech, Hypotonia) 6. Ear examination 7. Consider undertaking a HiNTS examination - for more on this have a look at this St Emlyns blogpost, the paper it references: doi.org/10.1016/j.annemergmed.2017.10.012 and these YouTube videos
8. For patients with suspected BPPV, consider undertaking a Dix-Hallpike and then Epley manoeuvre, for more information have a look at this EMJ letter: doi:10.1136/emj.2010.105874
CausesCentral
Want to know more?Please have a listen to this podcast from the excellent people over at FOAMcast Martin Dore
Clare Bosanko
4 Comments
7/11/2018 06:44:55
Good information, thank u and please visit back my article~! 17/11/2021 03:52:46
Very delighted to come across this useful blog. Aneurysms of the posterior circulation, including superior cerebellar artery (SCA) aneurysms, present unique technical challenges because they can only be accessed via maneuvering through deep operative corridors with limited working angles bound by critical neurovascular structures. For any further informations on stenting you may visit this article : https://bit.ly/3chdGlO 22/4/2024 11:17:18
Ein gut gestalteter Gartenzaun, Doppelstabmattenzaun, und Zaun kann die Schönheit des Gartens verbessern und als dekoratives Element dienen, das den Gesamtlook des Außenbereichs ergänzt. Leave a Reply. |
|
|